Summary
Background: Inflammation is increasingly recognized as an active contributor to the pathogenesis of hematological diseases rather than a secondary consequence. Persistent inflammatory signaling disrupts bone marrow homeostasis, alters immune regulation, and promotes disease progression.
Objective: This review evaluates the role of inflammation in hematological diseases, with particular emphasis on leukemia, highlighting molecular mechanisms, microenvironmental interactions, and clinical relevance.
Methods: A narrative review of peer-reviewed literature published between 2000 and 2024 was conducted using PubMed, Scopus, Web of Science, and Google Scholar. Relevant studies addressing inflammatory pathways, cytokine signaling, and hematological disease progression were analyzed.
Key Findings: Chronic elevation of pro-inflammatory cytokines, including interleukin-1, interleukin-6, and tumor necrosis factor-α, activates NF-κB and JAK/STAT signaling pathways, leading to leukemic cell survival, immune suppression, endothelial dysfunction, and inhibition of normal hematopoiesis. In leukemia, inflammation-driven interactions within the bone marrow microenvironment contribute to disease progression and therapeutic resistance. Inflammatory biomarkers such as C-reactive protein, interleukin-6, and endothelial activation markers demonstrate diagnostic and prognostic relevance. Similar inflammation-mediated mechanisms are also observed in non-malignant disorders, including anemia of chronic disease and myelodysplastic syndromes.
Conclusion: Inflammation plays a central role in the pathogenesis and clinical behavior of hematological diseases, particularly leukemia. Targeting inflammation-associated pathways alongside conventional therapies may improve disease management and clinical outcomes.
Keywords
Inflammation; Hematological disorders; Leukemia; Cytokines; Biomarkers.
Introduction
Hematological diseases comprise a broad spectrum of disorders affecting blood cells, bone marrow, and lymphoid organs, and they remain
a significant cause of morbidity and mortality worldwide despite advances in diagnosis and treatment [1,2].
These disorders include malignant conditions such as leukemia and lymphoma, as well as non-malignant disorders including anemia, thrombocytopenia, and other cytopenias arising from impaired hematopoiesis [1,2]. The clinical heterogeneity of hematological diseases reflects their complex etiology, which involves genetic abnormalities, environmental exposures, and immune-mediated mechanisms acting in concert [3]. Inflammation has emerged as an important biological link between immune dysregulation and hematological pathology, extending beyond its traditional role in host defense [3].
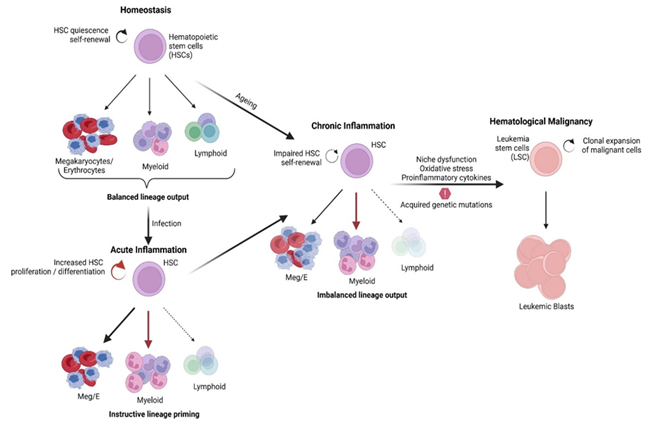
While acute inflammation is essential for pathogen clearance and tissue repair, persistent or dysregulated inflammatory responses can adversely affect hematopoietic function [1]. Chronic inflammatory signaling disrupts bone marrow homeostasis, alters stem and progenitor cell behavior, and contributes to ineffective blood cell production [2].
The bone marrow microenvironment plays a central role in maintaining normal hematopoiesis through interactions between hematopoietic cells, stromal cells, endothelial cells, and immune mediators [1]. Pro-inflammatory cytokines such as interleukin-1, interleukin-6, and tumor necrosis factor-α are key regulators of stress-induced hematopoiesis and immune activation within this niche [2]. Sustained exposure to these cytokines promotes stem cell exhaustion, lineage imbalance, and suppression of normal hematopoietic differentiation [3]. At the molecular level, chronic inflammation induces oxidative stress and excessive production of reactive oxygen species, leading to DNA damage and impaired genomic stability in hematopoietic cells [3]. Repeated inflammatory insults may overwhelm cellular repair mechanisms, thereby increasing susceptibility to leukemogenic mutations and clonal expansion [1].
These processes provide a mechanistic explanation for the association between chronic inflammatory conditions and the development of hematological malignancies [3]. In malignant hematological disorders, inflammation actively contributes to disease maintenance rather than representing a secondary consequence of tumor burden [3]. Malignant cells and surrounding immune cells engage in reciprocal signaling that reinforces inflammatory pathways, suppresses anti-tumor immune responses, and promotes cell survival [1,2]. This inflammatory feedback loop is particularly evident in leukemia, where it influences disease progression, immune evasion, and therapeutic resistance [3].
Recent advances in computational analysis and biomarker research have further emphasized the diagnostic and prognostic relevance of inflammation in hematological diseases [4]. Integration of inflammatory markers with conventional hematological parameters has improved disease classification and risk stratification [4]. These findings underscore the translational importance of understanding inflammation-driven mechanisms in hematological pathology [4]. This review aims to critically examine the role of inflammation in hematological diseases, with emphasis on underlying mechanisms, leukemic microenvironment interactions, and emerging diagnostic and therapeutic implications. By synthesizing current evidence, this article highlights inflammation as a central determinant of disease progression and clinical outcome in hematological disorders.
2. Literature search strategy.
This review was developed using a narrative literature approach to evaluate the role of inflammation in hematological diseases. A comprehensive search was performed using electronic databases including PubMed, Scopus, Web of Science, and Google Scholar. Articles published between 2000 and 2024 were considered. Search terms included combinations of inflammation, hematological diseases, leukemia, cytokines, bone marrow microenvironment, NF-κB, JAK/STAT, and inflammatory biomarkers. Selection was based on relevance to inflammatory mechanisms, disease progression, diagnostic value, and therapeutic implications.
Peer-reviewed original research articles, clinical studies, and review papers published in English were included. Conference abstracts, non-peer-reviewed sources, and studies lacking mechanistic or clinical relevance were excluded. Additional articles were identified through manual screening of reference lists from selected publications. This approach allowed integration of mechanistic, translational, and clinical perspectives related to inflammation-driven hematological pathology.
3. Mechanism of Inflammation in Hematological Diseases
Inflammation influences hematological diseases through a complex network of immune sensing, cytokine signaling, cellular activation, and intracellular regulatory pathways that collectively disrupt normal hematopoietic function [5]. These mechanisms involve coordinated interactions between innate and adaptive immune responses, linking early immune recognition to sustained inflammatory signaling within hematological tissues [6]. Dysregulation of these pathways shifts inflammation from a protective response to a disease-promoting process in the hematopoietic system [5].
3.1 Innate and Adaptive Immune Interface
The innate immune system initiates inflammatory responses by recognizing pathogen-associated and damage-associated molecular patterns through pattern recognition receptors such as Toll-like receptors and NOD-like receptors [5]. Activation of these receptors triggers the rapid release of cytokines and chemokines, leading to immune cell recruitment and amplification of inflammatory signaling [5]. Innate immune activation directly shapes adaptive immune responses by influencing antigen presentation, T-cell priming, and B-cell differentiation [6]. Evolutionary and functional studies indicate that innate and adaptive immunity operate as an integrated system rather than as separate entities [6]. Persistent activation of this immune interface in hematological diseases leads to prolonged inflammation and impaired immune regulation [5]. Such dysregulation contributes to ineffective immune surveillance and altered hematopoietic signaling [6].
3.2 Cellular Effectors: Neutrophils and Myeloid Cells
Neutrophils play an important role in inflammatory regulation beyond their classical function as short-lived phagocytic cells [7]. Activated neutrophils release cytokines, proteolytic enzymes, and reactive oxygen species that amplify local and systemic inflammatory responses [7]. The formation of neutrophil extracellular traps further sustains inflammation by exposing intracellular components that activate immune signaling pathways [7]. Myeloid cells, including monocytes and macrophages, act in concert with neutrophils to regulate the progression and resolution of inflammation [7]. In chronic inflammatory states, persistent activation of these cells disrupts tissue homeostasis and alters the bone marrow microenvironment [7]. Such alterations impair normal hematopoietic stem and progenitor cell function [7].
3.3 Cytokine Signaling and Systemic Communication
Pro-inflammatory cytokines such as interleukin-1, interleukin-6, and tumor necrosis factor family members serve as central mediators of inflammatory communication [8]. These cytokines exert both local effects within the bone marrow and systemic effects through circulation to distant organs [9]. Sustained cytokine signaling skews hematopoietic stem cell differentiation toward myeloid lineages and suppresses normal blood cell production [8]. Inflammatory cytokines also interact with the central nervous system through humoral and neural pathways [9]. This bidirectional neuroimmune communication reinforces chronic inflammatory states and influences systemic immune regulation [9]. Such feedback mechanisms contribute to the persistence of inflammation in hematological diseases [8].
3.4 Intracellular Signaling Pathways
Inflammatory signals converge on conserved intracellular signaling pathways that regulate cell survival, proliferation, and transcriptional activity [10]. Key pathways include MAPK/ERK and PI3K/AKT cascades, which integrate signals from cytokine receptors and immune sensors [10]. Persistent activation of these pathways promotes apoptosis resistance, differentiation arrest, and abnormal cell proliferation [5]. In hematopoietic and stromal cells, dysregulated intracellular signaling disrupts normal feedback control mechanisms [10]. This disruption allows inflammatory responses to persist beyond their physiological role [5]. Such maladaptive signaling directly contributes to hematological dysfunction and disease progression [10].
3.5 Integration and Pathological Outcomes
The biological outcome of inflammatory signaling depends on the balance between pro-inflammatory and regulatory mechanisms [5]. Acute and tightly regulated inflammation supports host defense, tissue repair, and immune homeostasis [7]. In contrast, chronic or uncontrolled inflammation leads to sustained cytokine production, immune cell activation, and microenvironmental remodeling [10]. In hematological diseases, these processes impair normal hematopoiesis, promote immune dysfunction, and create conditions favorable for malignant transformation [5]. Understanding these integrated mechanisms is essential for identifying therapeutic targets capable of interrupting inflammation-driven hematological pathology [8,10].
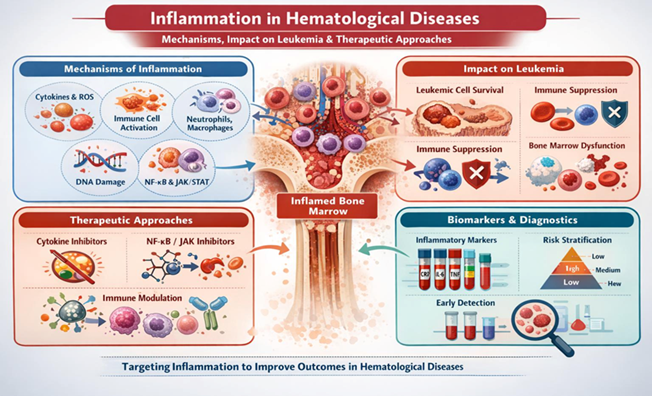
The integrated effects of chronic inflammatory signaling on hematopoietic cells, immune regulation, and the bone marrow microenvironment are summarized in Figure 1.
4. Role of Inflammation in Specific Hematological Disorder — Leukemia
Inflammation is now recognized as a fundamental component of the leukemic microenvironment, influencing disease initiation, progression, and response to therapy [11]. Leukemia development is not driven solely by intrinsic genetic alterations but is strongly shaped by extrinsic inflammatory signals within the bone marrow niche [12]. These inflammatory cues originate from immune cells, stromal elements, and endothelial cells, creating a microenvironment that favors leukemic cell survival [11,14].
Leukemic cells actively participate in sustaining inflammation by producing cytokines, chemokines, and growth factors that reinforce immune dysregulation [11]. This bidirectional interaction establishes a self-perpetuating inflammatory loop that promotes disease persistence and clonal expansion [12]. As a result, inflammation functions as both a driver and a consequence of leukemic burden [11].
4.1 Inflammatory Microenvironment and Leukemogenesis
Chronic inflammatory signaling contributes to leukemogenesis by enhancing the survival and expansion of pre-leukemic and leukemic clones [11]. Pro-inflammatory cytokines such as tumor necrosis factor-α, interleukin-1, and interleukin-6 activate transcriptional programs that promote resistance to apoptosis and uncontrolled proliferation [11]. These cytokines primarily exert their effects through activation of NF-κB and JAK/STAT signaling pathways, which are frequently dysregulated in leukemia [11]. Persistent inflammation also induces oxidative stress within hematopoietic progenitor cells [11]. Excessive generation of reactive oxygen species leads to DNA damage and increased genomic instability [11]. This inflammation-driven mutational pressure accelerates leukemic transformation and disease progression [11].
4.2 Cytokine-Mediated Immune Dysregulation
In acute myeloid leukemia, elevated levels of inflammatory cytokines are consistently observed and correlate with disease severity [12]. Cytokines such as interleukin-1β, interleukin-6, and tumor necrosis factor-α suppress cytotoxic T-cell function and impair natural killer cell activity [12]. This immune suppression facilitates leukemic immune evasion and limits effective anti-tumor responses [12]. Inflammatory cytokines also influence immune cell recruitment and polarization within the leukemic microenvironment [12]. Activation of monocytes, macrophages, and myeloid-derived suppressor cells further amplifies immunosuppressive signaling [14]. These changes contribute to immune exhaustion and reduced therapeutic efficacy [12].
4.3 Endothelial Dysfunction and Coagulation Abnormalities
Inflammation-induced endothelial activation represents an important pathological feature of leukemia [13]. Pro-inflammatory mediators disrupt endothelial integrity and increase expression of adhesion molecules within the bone marrow vasculature [13]. These alterations facilitate leukemic cell adhesion, migration, and retention within protective vascular niches [13]. In chronic lymphocytic leukemia, endothelial inflammation is closely associated with coagulation abnormalities and increased thrombotic risk [13]. Cytokine-mediated vascular injury, combined with immunomodulatory therapies, further exacerbates endothelial dysfunction [13]. This highlights the contribution of inflammation to both disease pathology and treatment-related complications [13].
4.4 Inflammation-Mediated Suppression of Normal Hematopoiesis
Leukemia-associated inflammation profoundly disrupts normal hematopoiesis within the bone marrow [14]. Inflammatory mediators released by leukemic cells impair hematopoietic stem and progenitor cell function [14]. This suppression contributes to anemia, neutropenia, and thrombocytopenia commonly observed in affected patients [14]. Activated immune cells within the leukemic niche further inhibit stem cell renewal and differentiation [14]. Over time, inflammation-driven remodeling of the bone marrow microenvironment leads to sustained hematopoietic failure [14]. These effects significantly worsen clinical outcomes and disease-related morbidity [14].
4.5 Clinical and Critical Perspective
Although extensive evidence links inflammation to leukemic progression, variability exists across studies regarding the prognostic value of individual inflammatory mediators [11]. Differences in leukemia subtype, disease stage, patient demographics, and treatment exposure contribute to inconsistent findings [12]. Furthermore, much of the available evidence is derived from observational studies or preclinical models, limiting direct causal interpretation [11]. Despite these limitations, inflammation remains a clinically relevant therapeutic target in leukemia [11]. Understanding the balance between protective immune responses and pathological inflammation is essential for optimizing treatment strategies [14]. An integrated view of inflammation-driven mechanisms is therefore critical for improving leukemia management and outcomes [11].
Figure 2 illustrates the key inflammatory pathways involved in leukemic progression, immune suppression, endothelial dysfunction, and potential therapeutic targets. Although leukemia represents a major focus of current research, inflammatory mechanisms are also implicated in several non-malignant and pre-malignant hematological conditions. In anemia of chronic disease, persistent interleukin-6 signaling induces hepcidin overexpression, leading to impaired iron availability and reduced erythropoiesis. Myelodysplastic syndromes and myeloproliferative neoplasms exhibit chronic immune activation within the bone marrow, where inflammatory cytokines contribute to ineffective hematopoiesis and clonal expansion. These observations suggest that inflammation acts as a common pathological denominator across diverse hematological disorders, reinforcing its broader clinical relevance beyond leukemia.
5. Therapeutic Implications of Inflammation in Leukemia.
The recognition of inflammation as a key driver of leukemic progression has expanded therapeutic strategies beyond direct cytotoxic targeting of malignant cells [11]. Persistent inflammatory signaling within the bone marrow microenvironment promotes leukemic cell survival, immune evasion, and resistance to conventional chemotherapy [12]. Targeting inflammation-associated pathways therefore represents a complementary approach to improve treatment outcomes in leukemia [11].
5.1 Cytokine-Targeted Therapeutic Strategies
Pro-inflammatory cytokines such as interleukin-1, interleukin-6, and tumor necrosis factor-α play a central role in sustaining leukemic cell growth and survival [12]. Pharmacological inhibition of interleukin-1 signaling using agents such as anakinra has demonstrated the ability to reduce inflammatory cytokine production and suppress leukemic proliferation in preclinical studies [15]. Similarly, blockade of interleukin-6 signaling has been shown to interfere with STAT3-mediated survival pathways in leukemic cells [15].
Targeting tumor necrosis factor-α has also been explored as a strategy to disrupt inflammation-driven leukemic signaling [13]. Inhibition of these cytokines can attenuate downstream activation of NF-κB and JAK/STAT pathways, thereby enhancing leukemic cell sensitivity to apoptosis [11]. In addition to anti-leukemic effects, cytokine-targeted therapies may reduce systemic inflammatory symptoms and improve patient quality of life [15].
5.2 NF-κB and JAK/STAT Pathway Inhibition
The NF-κB and JAK/STAT signaling pathways serve as major transcriptional regulators translating inflammatory signals into pro-survival gene expression programs in leukemia [11]. Constitutive activation of these pathways is frequently observed in both acute and chronic leukemias [15]. This dysregulation contributes to uncontrolled proliferation, resistance to apoptosis, and immune suppression [11]. JAK inhibitors such as ruxolitinib have demonstrated efficacy in suppressing cytokine-driven inflammatory signaling in hematological malignancies [11]. Proteasome inhibitors, including bortezomib, indirectly inhibit NF-κB activation by preventing degradation of inhibitory proteins [15]. Inhibition of these pathways disrupts leukemic–stromal interactions and enhances responsiveness to chemotherapy [14].
5.3 Anti-inflammatory and Immunomodulatory Approaches
Corticosteroids remain an integral component of leukemia treatment due to their potent anti-inflammatory and immunosuppressive properties [13]. These agents reduce cytokine production and induce apoptosis in selected leukemic subtypes [13]. However, long-term corticosteroid use is associated with metabolic, infectious, and cardiovascular complications, limiting their prolonged application [13]. Immunomodulatory drugs have demonstrated therapeutic benefit in selected hematological malignancies by altering immune cell activity and cytokine profiles [13]. In chronic lymphocytic leukemia, agents such as lenalidomide may paradoxically induce endothelial inflammation and increase thrombotic risk [13]. These observations highlight the complexity of inflammation-targeted therapies and the need for careful patient monitoring [13].
5.4 Targeting the Leukemic Microenvironment
Inflammation-driven remodeling of the bone marrow microenvironment plays a crucial role in leukemic stem cell survival and disease persistence [14]. Disruption of microenvironmental signaling aims to reduce niche-mediated drug resistance and immune suppression [14]. Targeting the CXCR4–CXCL12 axis has shown promise in mobilizing leukemic cells from protective niches and enhancing chemotherapy efficacy [15]. Reprogramming macrophage polarization and inhibiting myeloid-derived suppressor cell activity represent additional strategies to restore immune balance [14]. Reduction of inflammation-induced immune suppression may improve anti-leukemic immune responses and long-term diseae control [15]. These approaches underscore the therapeutic potential of targeting inflammation at the level of the tumor microenvironment [14].
5.5 Critical Perspective on Inflammation-Targeted Therapy
Despite encouraging results, inflammation-targeted therapies are not universally effective across all leukemia subtypes [11]. Heterogeneity in cytokine dependency, genetic background, and disease stage contributes to variable therapeutic responses [12]. Moreover, many anti-inflammatory strategies remain supported primarily by preclinical or early-phase clinical evidence [15]. Future therapeutic success will likely depend on patient-specific inflammatory profiling and rational combination strategies [11]. Integrating inflammation-targeted approaches with chemotherapy, targeted therapy, and immunotherapy may enhance efficacy while minimizing resistance [14]. A deeper understanding of inflammation-driven signaling networks is therefore essential for optimizing therapeutic interventions in leukemia [11].
6. Inflammatory Biomarkers and Diagnostic Relevance.
Inflammatory biomarkers provide valuable insight into disease activity, prognosis, and therapeutic response in hematological malignancies, particularly leukemia [16]. These biomarkers reflect the intensity of immune activation and the extent of microenvironmental disruption within the bone marrow [16]. Measurement of inflammatory mediators has therefore gained importance as an adjunct to conventional diagnostic and prognostic tools [16].
6.1 Cytokines as Diagnostic and Prognostic Indicators
Pro-inflammatory cytokines such as interleukin-6, interleukin-1β, and tumor necrosis factor-α are frequently elevated in patients with leukemia [12]. Elevated cytokine levels correlate with increased disease burden, aggressive clinical behavior, and reduced overall survival [12]. Interleukin-6 has been particularly associated with treatment resistance and adverse outcomes in acute leukemias [12]. Despite their clinical relevance, cytokine levels show considerable inter-patient variability [16]. Factors such as infection, therapy-related inflammation, and comorbid conditions can confound interpretation [16]. These limitations restrict the use of individual cytokines as standalone diagnostic markers [16].
6.2 Acute Phase Reactants and Systemic Inflammation Markers
Acute-phase proteins including C-reactive protein and ferritin serve as indirect indicators of systemic inflammation in hematological diseases [16]. Elevated levels of these markers are commonly observed in leukemic patients and often reflect active disease or inflammatory complications [16]. Hyperferritinemia has been associated with cytokine release syndromes and immune dysregulation in advanced disease stages [16]. However, acute-phase reactants lack disease specificity [16]. Their elevation may result from infections, transfusions, or treatment-related inflammation rather than leukemia itself [16]. Therefore, these markers are most informative when interpreted in conjunction with clinical and laboratory findings [16].
6.3 Cellular and Molecular Biomarkers
Inflammation-related signaling molecules such as NF-κB and STAT3 have emerged as molecular biomarkers of leukemic progression [11]. Persistent activation of these pathways is associated with enhanced leukemic cell survival and immune evasion [11]. Detection of pathway activation status may provide prognostic information and guide targeted therapeutic decisions [11]. Expression patterns of immune checkpoint molecules and inflammatory receptors also reflect immune dysregulation in leukemia [14]. Alterations in these markers may predict responsiveness to immunomodulatory and inflammation-targeted therapies [14]. Integration of molecular biomarkers into diagnostic workflows may improve personalized treatment strategies [14].
6.4 Emerging Biomarkers and Clinical Challenges
Recent studies have explored composite inflammatory indices combining cytokine levels, immune cell ratios, and acute-phase proteins [16]. Such integrated biomarker panels may provide greater prognostic accuracy than individual markers alone [16]. However, lack of standardization and assay variability remain significant obstacles to clinical implementation [16]. longitudinal monitoring of inflammatory biomarkers may offer insight into treatment response and early relapse detection [12]. Despite this potential, large-scale prospective studies are required to validate clinical utility [16]. Careful interpretation of inflammatory biomarkers is therefore essential to avoid overestimation of their diagnostic value [16].
7. Future Perspectives and Research Directions.
Growing evidence indicates that inflammation is not merely a secondary feature of hematological diseases but an active contributor to disease initiation and progression [17]. Future research must focus on delineating the temporal relationship between inflammatory signaling and genetic alterations in hematopoietic cells [17]. Clarifying this relationship may help identify early intervention points before irreversible malignant transformation occurs [17]. Advances in single-cell sequencing and spatial transcriptomics offer new opportunities to dissect inflammatory heterogeneity within the bone marrow microenvironment [17]. These technologies can reveal cell-specific inflammatory signatures that are not captured by bulk analyses [17]. Such insights may improve risk stratification and therapeutic targeting in leukemia and related disorders [17]. Identification of reliable inflammation-based biomarkers remains a critical research priority [16]. Standardization of assay methods and validation across diverse patient cohorts are essential for clinical translation [16]. Future studies should emphasize longitudinal biomarker monitoring to better predict treatment response and relapse [16].
The development of combination therapies targeting both leukemic cells and inflammatory pathways represents a promising direction [15]. Rational integration of anti-inflammatory agents with chemotherapy, targeted therapy, or immunotherapy may enhance efficacy while limiting resistance [15]. However, careful evaluation of immunosuppressive risks is required to avoid compromising host defense [15]. Finally, expanding research beyond leukemia to include other hematological diseases such as myelodysplastic syndromes and myeloproliferative neoplasms will improve alignment between title and content [17]. Comparative studies across disease entities may uncover shared inflammatory mechanisms and disease-specific differences [17]. Such approaches are essential for developing broadly applicable and disease-tailored therapeutic strategies [17].
Conclusion
Inflammation has emerged as a fundamental driver of hematological disease pathogenesis, extending beyond a secondary response to malignant transformation or tissue injury. In leukemia and related disorders, sustained inflammatory signaling reshapes the bone marrow microenvironment, promotes leukemic cell survival, and suppresses normal hematopoiesis through persistent activation of cytokine-mediated pathways such as NF-κB and JAK/STAT. These processes contribute to immune dysfunction, endothelial activation, and therapeutic resistance, collectively worsening clinical outcomes.
Recognition of inflammation as a dynamic component of disease biology has important translational implications. Targeting inflammatory pathways alongside conventional cytotoxic and targeted therapies may enhance treatment efficacy and reduce disease persistence. In parallel, inflammatory biomarkers including interleukin-6, C-reactive protein, and markers of endothelial activation hold promise for improving diagnosis, prognostication, and treatment monitoring. Continued integration of inflammation-focused research into clinical practice may support more precise, mechanism-based management strategies for hematological diseases.
Conflict of interest statement
Not applicable
Acknowledgment
The authors would like to express their sincere appreciation to the faculty and management of B. R. Harne College of Pharmacy, Karav, Vangani, for providing the academic support and institutional facilities required for the successful completion of this review article. The guidance and constructive suggestions offered by the teaching staff were instrumental in improving the scientific depth and clarity of the manuscript.
The authors gratefully acknowledge the contributions of researchers and scholars whose previously published studies formed the scientific foundation of this review. Access to peer-reviewed journals, academic databases, and open-access scientific resources played a vital role in the collection, analysis, and interpretation of relevant literature.
The authors also acknowledge the academic environment that encouraged critical discussion and scholarly exchange, which contributed to refining the conceptual framework of the article. No specific funding was received for this work, and the authors declare that the preparation of this manuscript was carried out independently, without any external financial support.
References
- Murphy MF, Stanworth SJ. Haematological disease. In: Murphy MF, Stanworth SJ, editors. Practical Transfusion Medicine. 3rd ed. Oxford: Wiley-Blackwell; 2009. p. 308–319.
- McKew S, Bates I, Olayemi E. Hematologic diseases. In: Ryan ET, Hill DR, Solomon T, Aronson NE, Endy TP, editors. Hunter’s Tropical Medicine and Emerging Infectious Diseases. 10th ed. Philadelphia: Elsevier; 2020. p. 34–43.
- Milton JG, Mackey MC. Periodic haematological diseases: mystical entities or dynamical disorders? J R Coll Physicians Lond. 1989;23(4):236–240.
- Gunčar G, Kukar M, Notar M, Brvar M, Černelč P, Notar M. An application of machine learning to haematological diagnosis. Sci Rep. 2018;8(1):411.
- Janeway CA Jr, Travers P, Walport M, Shlomchik MJ. Principles of innate and adaptive immunity. In: Immunobiology: The Immune System in Health and Disease. 5th ed. New York: Garland Science; 2001.
- Flajnik MF, Du Pasquier L. Evolution of innate and adaptive immunity: can we draw a line? Trends Immunol. 2004;25(12):640–644.
- Mantovani A, Cassatella MA, Costantini C, Jaillon S. Neutrophils in the activation and regulation of innate and adaptive immunity. Nat Rev Immunol. 2011;11(8):519–531.
- Dantzer R, Aubert A, Bluthé RM, Gheusi G, Cremona S, Layé S, et al. Mechanisms of the behavioural effects of cytokines. In: Cytokines, Stress, and Depression. New York: Springer; 2007. p. 83–105.
- Licinio J, Wong ML. Pathways and mechanisms for cytokine signaling of the central nervous system. J Clin Invest. 1997;100(12):2941–2947.
- Meroni SB, Galardo MN, Rindone G, Gorga A, Riera MF, Cigorraga SB. Molecular mechanisms and signaling pathways involved in Sertoli cell proliferation. Front Endocrinol (Lausanne). 2019;10:224.
- Krawczyk J, O’Dwyer M, Swords R, Freeman C, Giles FJ. The role of inflammation in leukaemia. In: Aggarwal BB, Sung B, Gupta SC, editors. Inflammation and Cancer. Basel: Springer; 2014. p. 335–360.
- Zhong FM, Yao FY, Liu J, Zhang HB, Li MY, Jiang JY, et al. Inflammatory response mediates cross-talk with immune function and reveals clinical features in acute myeloid leukemia. Biosci Rep. 2022;42(5):BSR20220647.
- Aue G, Nelson Lozier J, Tian X, Cullinane AM, Soto S, Samsel L, et al. Inflammation, TNF-α and endothelial dysfunction link lenalidomide to venous thrombosis in chronic lymphocytic leukemia. Am J Hematol. 2011;86(10):835–840.
- Cui P, Zhang Y, Cui M, Li Z, Ma G, Wang R, et al. Leukemia cells impair normal hematopoiesis and induce functional loss of hematopoietic stem cells through immune cells and inflammation. Leuk Res. 2018;65:49–54.
- Récher C. Clinical implications of inflammation in acute myeloid leukemia. Front Oncol. 2021;11:623952.
- Huang LW, Olin RL. Inflammatory biomarkers and patient-reported outcomes in acute myeloid leukemia: refocusing on older adults. J Geriatr Oncol. 2020;11(3):395–398.
- Smith MT, McHale CM, Wiemels JL, Zhang L, Wiencke JK, Zheng S, et al. Molecular biomarkers for the study of childhood leukemia. Toxicol Appl Pharmacol. 2005;206(2):237–245.
- Sulicka J, Surdacki A, Mikołajczyk T, Strach M, Gryglewska B, Ćwiklińska M, et al. Elevated markers of inflammation and endothelial activation in adult survivors of childhood acute lymphoblastic leukemia. Immunobiology. 2013;218(5):810–816.
- Saluja S, Bansal I, Bhardwaj R, Beg MS, Palanichamy JK. Inflammation as a driver of hematological malignancies. Front Oncol. 2024 Mar 20;14:1347402. doi:10.3389/fonc.2024.1347402.

